Blank DD 2870 Template
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," plays a crucial role in the healthcare process for military personnel and their families. This form is designed to authorize the release of medical or dental records, ensuring that service members can access necessary care while maintaining the confidentiality of their health information. It serves as a bridge between healthcare providers and the military, facilitating the sharing of vital information when needed. Whether a service member is seeking treatment, transferring care, or pursuing benefits, the DD 2870 form is essential for ensuring that all parties involved have the necessary permissions in place. By understanding how to properly fill out and submit this form, individuals can navigate the often-complex healthcare landscape with greater ease and confidence.
Document Example
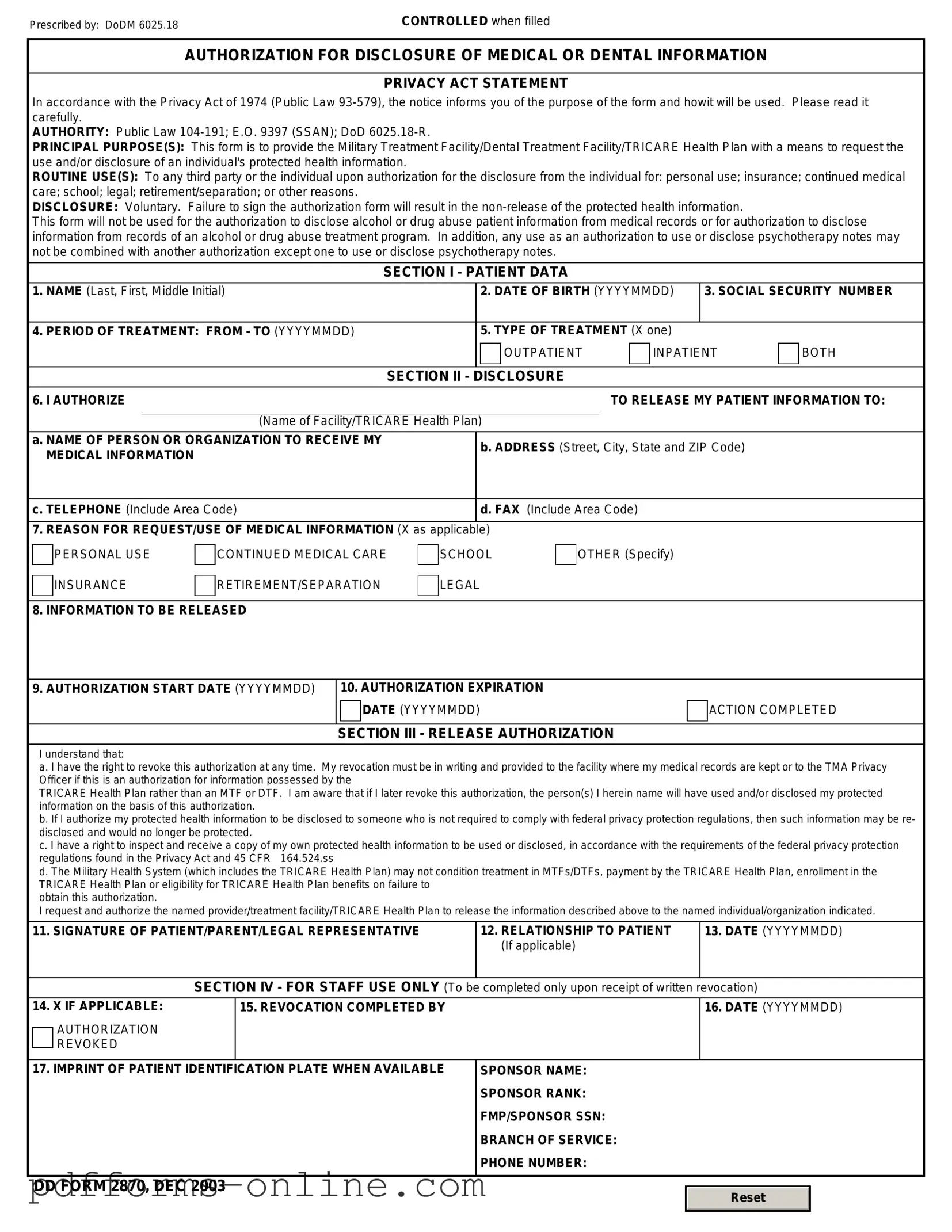
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Frequently Asked Questions
-
What is the DD 2870 form?
The DD 2870 form is a document used by the U.S. Department of Defense. It is specifically designed for service members and their families to request a copy of their medical records or to authorize the release of their medical information. This form ensures that individuals have access to their health records and can share this information with other healthcare providers if necessary.
-
Who needs to fill out the DD 2870 form?
Any service member, veteran, or eligible family member who wishes to obtain their medical records or authorize the release of medical information must complete the DD 2870 form. This includes active duty personnel, reservists, retirees, and dependents. It is important for individuals to understand that they must be the ones to request their records or provide authorization for someone else to do so on their behalf.
-
How do I complete the DD 2870 form?
To complete the DD 2870 form, individuals should follow these steps:
- Obtain a copy of the form, which can usually be found online or at military medical facilities.
- Fill in personal information, including name, Social Security number, and contact details.
- Specify the type of records being requested or the individual to whom the records should be released.
- Sign and date the form to confirm the request or authorization.
It is crucial to ensure that all information is accurate and complete to avoid delays in processing the request.
-
Where do I submit the DD 2870 form?
After completing the DD 2870 form, it should be submitted to the appropriate military medical facility or records office. The submission process may vary depending on the location and the specific requirements of the facility. It is advisable to check with the facility for any specific instructions regarding submission methods, such as in-person delivery, mailing, or electronic submission.
-
How long does it take to process the DD 2870 form?
The processing time for the DD 2870 form can vary. Generally, it may take anywhere from a few days to several weeks, depending on the volume of requests being handled by the medical facility. If there are any issues with the request, such as missing information, this may further delay processing. It is recommended to follow up with the facility if there are concerns about the status of the request.
Misconceptions
The DD 2870 form, often encountered in military and veteran contexts, is subject to several misconceptions. Below is a list that clarifies these misunderstandings.
- It is only for service members. Many believe that the DD 2870 form is exclusively for active duty personnel. In reality, this form is also applicable to veterans and their dependents, allowing them to request medical records or other pertinent information.
- It guarantees access to all medical records. Some assume that submitting the DD 2870 will automatically grant them access to all their medical records. However, access may be limited based on privacy regulations and the type of records requested.
- Filling it out is unnecessary for routine requests. A common misconception is that informal requests for records do not require the DD 2870. In most cases, a formal request using this form is necessary to ensure proper processing and compliance with regulations.
- It can be submitted in any format. Many individuals think that they can submit the DD 2870 in any format they choose. This is incorrect; the form must be completed as prescribed by the Department of Defense and submitted in its official format.
- There is no deadline for submission. Some believe that they can submit the DD 2870 at any time without consequence. However, there may be deadlines associated with specific requests, especially when related to benefits or claims.
Common mistakes
When filling out the DD 2870 form, individuals often encounter challenges that can lead to mistakes. Understanding these common errors can help ensure that the form is completed accurately and efficiently. Here are five mistakes to watch out for:
-
Incomplete Information: One of the most frequent errors is failing to provide all required information. Each section of the form must be filled out completely. Missing details can delay processing or result in a rejection of the application.
-
Incorrect Personal Information: It's essential to double-check personal details such as names, Social Security numbers, and addresses. Even a small typo can lead to significant complications.
-
Not Signing the Form: Many people forget to sign the DD 2870 form. A signature is a critical component that validates the information provided. Without it, the form is considered incomplete.
-
Failing to Read Instructions: Skimming through the instructions can lead to misunderstandings. Taking the time to read and understand the guidelines ensures that each section is completed correctly.
-
Submitting Without a Review: Rushing to submit the form without a thorough review can result in overlooking errors. It's advisable to take a moment to go over the completed form before sending it off.
By being mindful of these common mistakes, individuals can improve their chances of successfully completing the DD 2870 form. Accuracy and attention to detail are key to navigating this important process smoothly.
Additional PDF Templates
High School Transcript - Transcripts often reflect any awarded diplomas or certificates.
To create a comprehensive estate plan, individuals in Texas can utilize a Texas Last Will and Testament form, which can be easily found at OnlineLawDocs.com. This essential document ensures that one’s wishes regarding property and asset distribution are clearly articulated, thus guiding loved ones and executors in fulfilling those final intentions.
Class a Cdl Pre Trip Inspection Pictures - Clearly defined inspection phases help streamline the process.
Document Data
| Fact Name | Description |
|---|---|
| Form Title | DD Form 2870 is known as the Authorization for Disclosure of Medical or Dental Information. |
| Purpose | This form is used to authorize the release of medical or dental records for military personnel and their dependents. |
| Who Uses It | Active duty service members, retirees, and eligible family members may use this form. |
| Governing Law | The use of DD Form 2870 is governed by the Health Insurance Portability and Accountability Act (HIPAA) and Department of Defense regulations. |
| Submission Process | The completed form must be submitted to the appropriate medical facility or dental clinic. |
| Information Required | Individuals must provide personal information, including their name, Social Security number, and contact details. |
| Duration of Authorization | The authorization remains valid until the individual revokes it or the specified expiration date is reached. |
| Revocation Process | To revoke the authorization, a written notice must be submitted to the facility that received the original form. |
| Privacy Protections | Information disclosed under this form is protected under federal privacy laws and must be handled with confidentiality. |
Similar forms
The DD Form 214 is a document that serves as a Certificate of Release or Discharge from Active Duty. Like the DD 2870, which is used to request medical records, the DD 214 provides essential information about a service member's time in the military. It includes details such as the dates of service, type of discharge, and any awards or decorations received. Both forms are crucial for veterans seeking benefits, as they establish eligibility and provide a record of service history.
For those looking to secure a rental property, understanding the New York Residential Lease Agreement is essential, as it outlines the relationship between landlords and tenants. This document ensures that all parties are aware of their rights and responsibilities, covering aspects like rental payments and lease duration. For further insights and a comprehensive overview, you can refer to the documentonline.org/blank-new-york-residential-lease-agreement.
The VA Form 21-526EZ is another important document, specifically used to apply for disability compensation. Similar to the DD 2870, this form requires the submission of personal information and details about the service member's medical conditions. Both forms are designed to facilitate access to benefits, ensuring that veterans can receive the support they need based on their service and health status.
The SF 180, Request Pertaining to Military Records, is a form that allows individuals to request copies of their military records. This document is akin to the DD 2870 in that it seeks to obtain important records related to a service member's time in the military. Both forms help veterans and their families access vital information, whether for personal use or to apply for benefits, ensuring that they have the necessary documentation to support their claims.
The VA Form 21-4142 is used to authorize the release of medical information to the Department of Veterans Affairs. This form is similar to the DD 2870 in that it deals with medical records, allowing veterans to provide consent for the VA to obtain their health information. Both documents play a critical role in the claims process, as they help streamline the acquisition of medical records necessary for evaluating claims and benefits.